The Medical Mnemonic Handbook: MSK & Rheumatology Mastery Guide
Mastering Musculoskeletal (MSK) and Rheumatology board topics requires a transition from rote memorization to high-fidelity cognitive anchoring. This clinical guide utilizes Dual Coding Theory to link abstract immunological data to robust visual “mental pegs.” We provide the structural framework necessary to “see” the diagnosis before the labs return.
1. Connective Tissue Foundations: The Semantic Core
Rheumatology is the study of molecular mimicry and immune dysregulation within connective tissues. Mastery involves distinguishing between localized mechanical degradation and systemic autoimmune cascades. In this context, we define Systemic Autoimmune Rheumatic Diseases (SARDs) as chronic conditions where the loss of self-tolerance leads to multiorgan inflammatory damage, primarily targeting synovial joints, skin, and vascular structures.
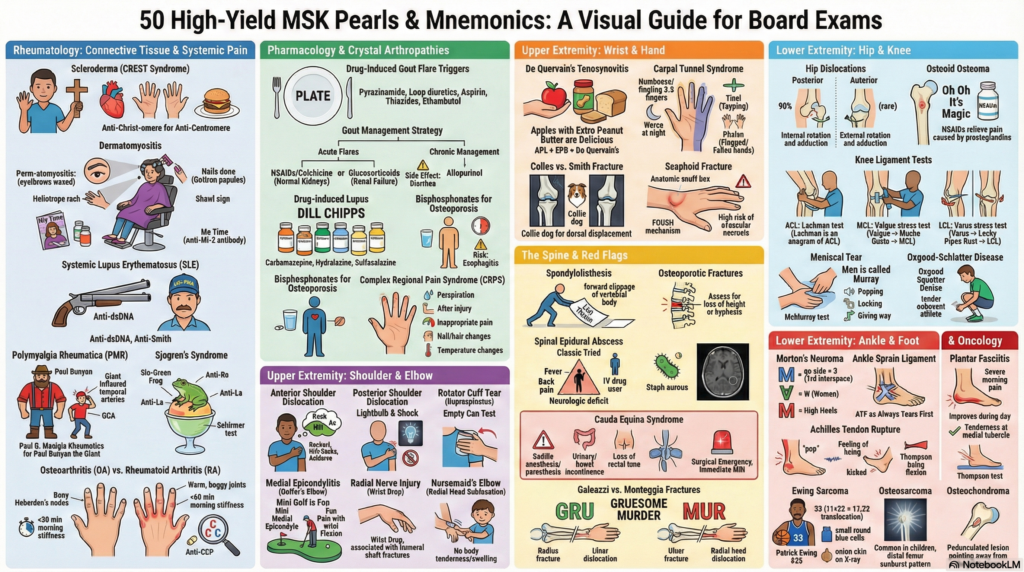
Identify pathognomonic visual signs (e.g., Heliotrope rash, Gottron papules).
Link symptoms to triggers (e.g., FOOSH for scaphoid fractures).
Apply high-specificity markers (e.g., Anti-CCP for Rheumatoid Arthritis).
2. Mechanistic Analysis: The Lupus & Gout Cascades
The pathophysiology of Systemic Lupus Erythematosus (SLE) centers on the failure to clear apoptotic debris. This results in an accumulation of nuclear antigens, triggering the production of Antinuclear Antibodies (ANA). Specifically, Anti-Smith and Anti-dsDNA represent the “smoking gun” of SLE, indicating highly specific double-stranded DNA destruction.
In contrast, Crystal Arthropathies like Gout are metabolic failures. Hyperuricemia leads to the precipitation of monosodium urate crystals in synovial fluid. These crystals act as Danger-Associated Molecular Patterns (DAMPs), activating the NLRP3 inflammasome, which recruits neutrophils and releases IL-1β, causing the excruciating pain of the “Great Toe” flare.
Mechanism Flow: Acute Gout Flare
3. The Dr. Belh Framework: Applied Clinical Mnemonics
A. The “Lou-Piss” Lupus Mastery
Observation: Visualize a man named Lou-Pissing on a Smith & Wesson Double Barrel shotgun. This anchors Anti-Smith and Anti-dsDNA as specific markers for SLE. ANA is your sensitivity screen; Lou’s shotgun is your specificity confirmation.
B. Dermatomyositis Salon
Context: “Perm-atomyositis.” Imagine a woman getting a perm at a salon. The Heliotrope rash is her eyebrow wax, Gottron papules are her manicure, and the Shawl sign is her salon cape. This anchors the Anti-Mi-2 (Me-time) antibody specificity.
C. The Stiffness Showdown (OA vs. RA)
Solution: Differentiating mechanical vs. inflammatory stiffness. Remember SpeCiFiC (two Cs) for Anti-CCP specificity in Rheumatoid Arthritis.
| Feature | Osteoarthritis (OA) | Rheumatoid Arthritis (RA) |
|---|---|---|
| Morning Stiffness | < 30 mins | > 60 mins |
| Joint Character | Hard and Bony (Nodes) | Warm and Boggy (Synovitis) |
| Pathophysiology | Mechanical Wear | Autoimmune Destruction |
4. Regional MSK: Critical Nerve & Bone Profiles
In the upper extremity, 90% of shoulder dislocations are Anterior (Antonio). He poses abducted and externally rotated, holding an Ax (Axillary nerve risk). Conversely, Posterior dislocations follow seizures or shocks, presenting with the Lightbulb sign on X-ray.
In oncology, the Patrick Ewing Sarcoma mnemonic is definitive. Translocation 11:22 (11+22=33, Ewing’s number), Small Blue Cells (The Jersey), and Onion Skinning (The Snack). This is high-yield clinical synthesis.
Treatment Efficacy Timeline: Rheumatoid Arthritis
Week 0
NSAIDs for Symptom Control
Week 4
DMARDs (Methotrexate) Peak
Week 12
Biologics Assessment (TNF-α)
5. Extraction Zone: Key Points for Boards
- Gout PLATE: Pyrazinamide, Loop Diuretics, Aspirin, Thiazides, Ethambutol (Triggers).
- Scaphoid: Snuffbox tenderness = Retrograde flow risk = Avascular Necrosis danger.
- Cauda Equina: Surgical emergency; Saddle Anesthesia + Loss of Rectal Tone = MRI Now.
- Scleroderma: “Anti-Christ-omere” (Anti-Centromere) for Limited/CREST syndrome.
- Lachman Test: Most sensitive for ACL (A-C-L is inside L-A-C-H-M-A-N).
6. The Medical Mnemonic MSK & Rheumatology Edition
7. Expert FAQ: Quick Clinical Hits
Q: What is the most sensitive test for SLE?
A: ANA (Antinuclear Antibody). If negative, SLE is highly unlikely.
Q: Why use Colchicine for acute gout?
A: It inhibits microtubule polymerization, preventing neutrophil migration to crystals.
Q: How do you differentiate a Smith vs. Colles fracture?
A: Direction of displacement. Colles is Dorsal (Collie Dog), Smith is Volar (Palmar).
Q: What is the pathognomonic sign of Dermatomyositis on the hands?
A: Gottron papules (violaceous papules on the knuckles).
Q: What is the lightbulb sign?
A: It represents a posterior shoulder dislocation on X-ray due to internal rotation of the humerus.