Mood Regulation and the Serotonin System: A Comparative Guide
By Dr. Belh
The serotonin system constitutes the fundamental neurological architecture of emotional equilibrium. Deficits in this pathway are central to clinical depression, yet resolution requires a precise distinction between neurotransmitter retention and biological synthesis. This article provides a rigorous mapping of these pathways.
1. Neurobiological Foundations: The 5-HT Pathway
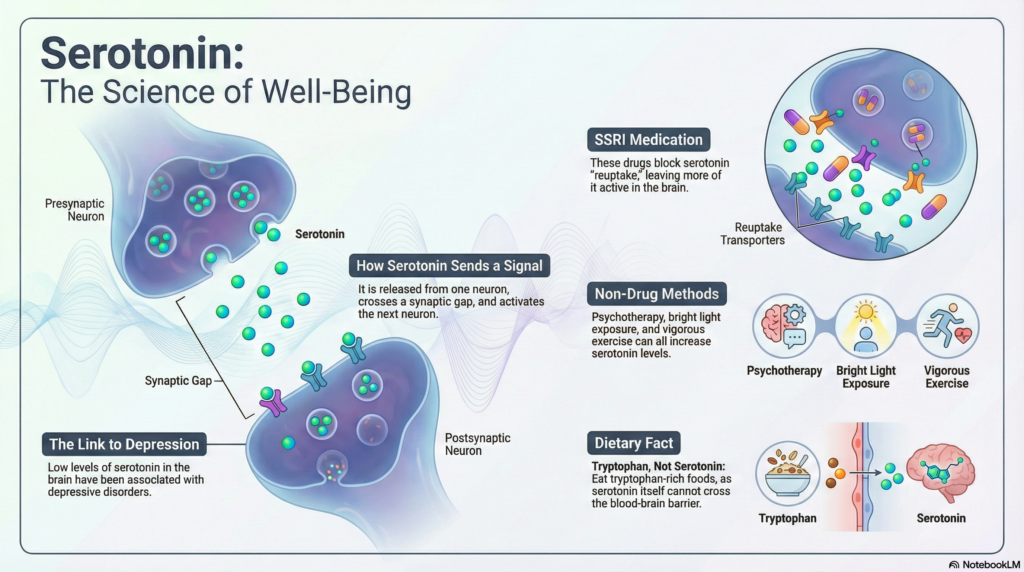
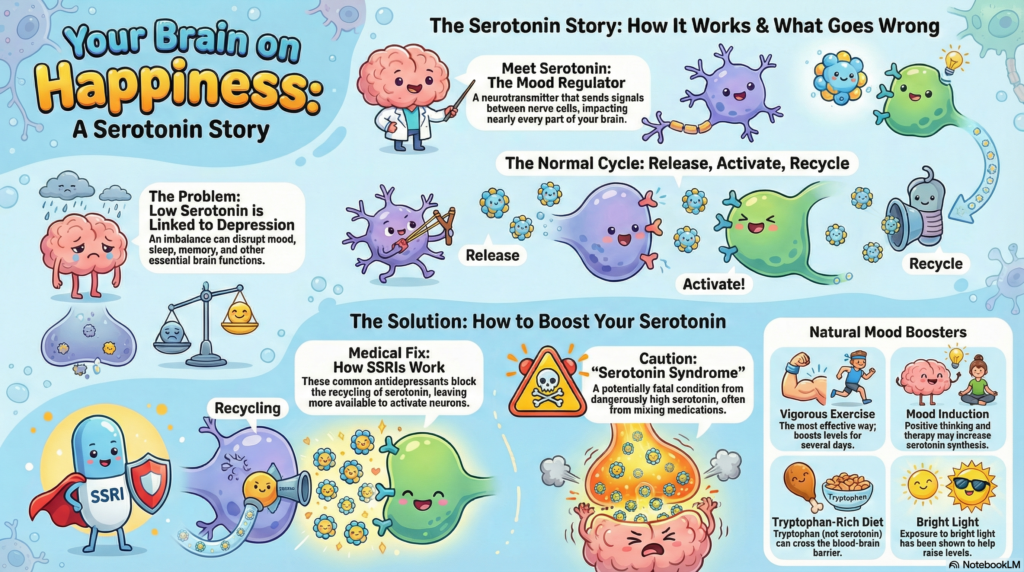
Serotonin, technically identified as 5-hydroxytryptamine (5-HT), is a monoamine neurotransmitter that operates as a master regulator of the central nervous system. Its synthesis originates primarily in the Raphe nuclei of the midbrain and brainstem. From this nexus, serotonergic neurons project to nearly every region of the brain, including the prefrontal cortex—the seat of executive function—and the limbic system, which governs emotional response.
Beyond mood stabilization, serotonin is intrinsically linked to the circadian rhythm (as a precursor to melatonin), satiety signals in the hypothalamus, and nociception (pain perception). A critical clinical distinction must be made regarding the Blood-Brain Barrier (BBB): while the enteric nervous system (gut) produces approximately 90% of the body’s serotonin, this peripheral serotonin cannot cross the BBB. Therefore, cognitive and emotional health depend entirely on the brain’s internal synthesis using the precursor amino acid L-Tryptophan.
Balances emotional valency and prevents extreme volatility in mood states.
Governs sleep cycles by regulating the transition from serotonin to melatonin.
Facilitates neuroplasticity and memory consolidation in the hippocampus.
2. Mechanistic Analysis: The Role of SSRIs
Selective Serotonin Reuptake Inhibitors (SSRIs) are the current pharmacological “gold standard” for depressive disorders. Their function is purely reductive of loss rather than productive of gain. In a healthy synapse, serotonin is released, binds to receptors (such as the 5-HT1A receptor), and is then recycled back into the pre-synaptic neuron via the Serotonin Transporter (SERT).
In clinical depression, this recycling occurs too efficiently, or the initial release is insufficient, leading to a “starved” synapse. SSRIs block the SERT protein, preventing reuptake. This results in an increased concentration of serotonin in the synaptic cleft, prolonging the signal duration. This sustained signaling eventually triggers downstream effects, including the expression of BDNF (Brain-Derived Neurotrophic Factor), which is the actual driver of mood improvement over a 4 to 8-week period.
THE SSRI ACTION CYCLE
3. Natural Synthesis Pathways: Non-Pharmacological Stimulation
While SSRIs focus on retention, natural interventions target Synthesis (Production). This is a vital clinical distinction. Research in neurobiology highlights three primary triggers for endogenous serotonin production:
- Vigorous Physical Exercise: Aerobic activity increases the ratio of tryptophan to other amino acids in the blood, facilitating its transport across the BBB. The resulting serotonin spike persists significantly longer than the activity itself.
- Bright Light Exposure: Retinal perception of high-intensity light (ideally >10,000 lux) triggers immediate serotonin synthesis, a mechanism frequently leveraged in treating Seasonal Affective Disorder (SAD).
- Mood Induction & Psychotherapy: Cognitive-behavioral shifts toward positive affect have been shown via PET scans to correlate with increased 5-HT synthesis, suggesting that biology and psychology exist in a reciprocal loop.
4. The Dr. Belh Framework: Integrated Clinical Protocol
To optimize mood regulation, I propose a three-tiered clinical approach:
5. Comparative Synthesis: Retention vs. Production
| Intervention | Biological Target | Duration of Effect | Status |
|---|---|---|---|
| SSRIs | SERT Protein (Retention) | Temporary (Requires Daily Dose) | Pharmacological |
| Exercise | Precursor Transport (Synthesis) | Semi-Permanent (Several Days) | Natural |
| Phototherapy | Ocular Trigger (Synthesis) | Immediate / Circadian | Environmental |
6. Featured Visual Concept (Prompt)
7. Clinical FAQ: Understanding the Nuances
Q1: Why is Tryptophan important if I’m taking SSRIs?
A: SSRIs only keep existing serotonin in the synapse. If your brain lacks the Tryptophan to produce serotonin in the first place, the medication has nothing to work with. Think of Tryptophan as the “fuel” and SSRIs as “sealing the leaks” in the tank.
Q2: What are the early signs of Serotonin Syndrome?
A: Agitation, rapid heart rate, dilated pupils, and muscle rigidity. It is a medical emergency caused by excessive serotonergic activity, often due to drug interactions.
Q3: Can lifestyle changes truly replace medication?
A: In cases of mild-to-moderate depression, lifestyle shifts (exercise, light, therapy) are statistically as effective as SSRIs. However, in severe major depression, medication is often a non-negotiable stabilizer.
Q4: How does the gut influence my brain’s serotonin?
A: While gut serotonin doesn’t cross into the brain, the gut microbiome produces precursors and influences the Vagus nerve, which communicates directly with the brain’s emotional centers.
Q5: Why is exercise more persistent than light therapy?
A: Exercise triggers complex metabolic shifts that improve the efficiency of the tryptophan-to-serotonin conversion for several days, whereas light therapy is primarily a momentary stimulus of the synthesis trigger.