Cortisol acts as the body’s primary energy deployment signal rather than a mere marker of psychological stress. Optimization of this hormone requires engineering a distinct circadian signature: a robust, sharp morning peak followed by a steep evening decline. This clinical guide outlines the mechanistic levers required to architect this rhythm for sustained cognitive performance and physiological recovery.
Clinical Contents
Definition: The HPA Axis Architecture
The Hypothalamic-Pituitary-Adrenal (HPA) axis constitutes the neuroendocrine command center for energy regulation. It operates via a negative feedback loop designed to maintain homeostasis.
Anatomically, the system functions as a cascade: the Hypothalamus (PVN) detects state requirements and releases CRH; this signals the Pituitary to release ACTH, which subsequently prompts the Adrenal glands to synthesize and secrete cortisol. The system is self-limiting; high circulating cortisol signals the PVN to cease production.
HPA Axis Feedback Loop
Releases CRH
Releases ACTH
Secrete CORTISOL
Mechanistic Analysis: The 24-Hour Rhythm
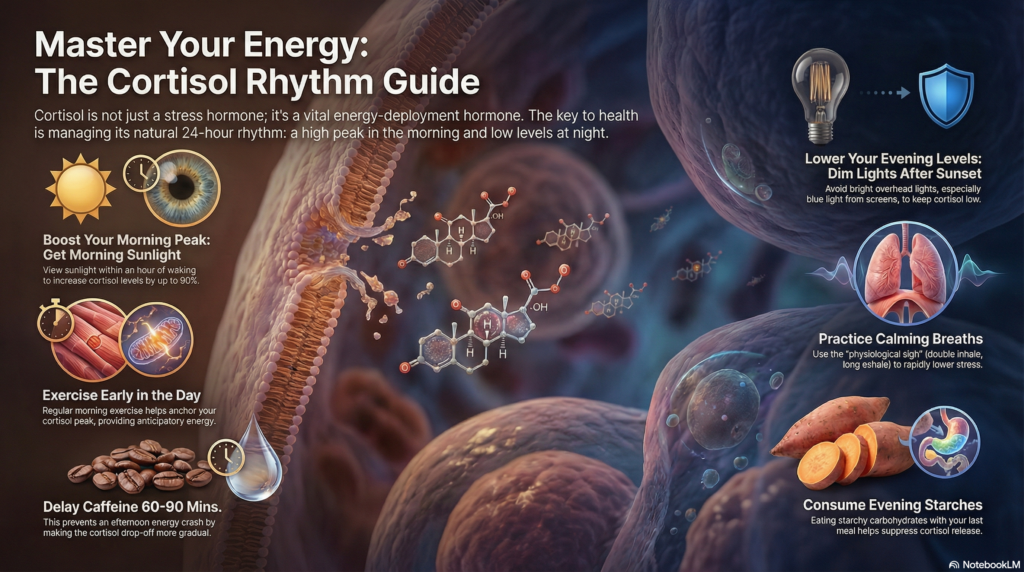
A healthy cortisol profile is defined by amplitude and timing. The biological imperative is the Cortisol Awakening Response (CAR): a 50% increase in cortisol levels within 30-60 minutes of waking. This surge functions as the metabolic “boot sequence” for the brain and body.
Conversely, the evening profile demands a steep decline. The nadir (lowest point) must occur during the first phase of sleep to facilitate growth hormone release and immune system repair. Dysregulation occurs when the curve flattens: the morning peak is blunted, and the evening decline fails.
Ideal Cortisol Circadian Arc
Applied Approach: The Dr. Belh Framework
1. Observation
Assess rhythm integrity. Do you experience morning inertia? This suggests a failed CAR. Do you experience evening alertness (“wired but tired”)? This indicates failed evening clearance.
2. Context (Zeitgebers)
Light is the primary time-giver. The SCN is hardwired to ocular input. High lux input (sunlight) triggers morning release; low Kelvin/lux input triggers evening suppression.
3. Solution Protocols
Intervention must be biphasic: Aggressive stimulation in the AM (Light + Hydration) and aggressive reduction in the PM (Dimming + Glucose + NSDR).
The Morning Protocol: Amplification
The objective is to maximize the amplitude of the waking pulse. This requires immediate interaction with the Suprachiasmatic Nucleus (SCN).
- Photon Exposure: 10-30 minutes of sunlight within 60 minutes of waking. If natural light is unavailable, use a 10,000 lux therapy lamp.
- Caffeine Delay: Delay ingestion by 90 minutes. This allows adenosine clearance to occur naturally, preventing the mid-afternoon crash.
- Hydration: Rehydrate immediately to support adrenal pulsatility.
The Evening Protocol: Clearance
The objective is to lower the “floor” of cortisol to enable melatonin onset.
- Light Hygiene: Eliminate overhead lighting and blue spectra (screens) 2 hours pre-bed.
- Glucose Timing: Starchy carbohydrates at dinner elevate blood glucose, which naturally suppresses cortisol (insulin/cortisol antagonism).
- Physiological Sigh: Mechanical ventilation control (double inhale, long exhale) to manually engage the parasympathetic system.
Burnout Classification & Recovery
Burnout is not “adrenal fatigue” (absence of cortisol) but rather rhythm dysregulation. It presents in two distinct phenotypes requiring opposing interventions.
Type 1: The Anxious Phenotype
Symptoms: Waking anxiety, early peaks, afternoon crash.
Intervention: Immediate Non-Sleep Deep Rest (NSDR) upon waking to blunt the premature spike, followed by delayed light exposure.
Type 2: The Flat Phenotype (“Sluggish”)
Symptoms: Morning brain fog, evening wakefulness.
Intervention: The pathology lies in the evening. High evening cortisol prevents the system from resetting. The cure for a sluggish morning is rigorous evening cortisol suppression.
Key Clinical Takeaways
- ✓
The morning peak is not optional; it dictates the slope of the daily curve. - ✓
Light is the primary drug. Use it with dosage precision (high lux AM, zero lux PM). - ✓
Caffeine does not give energy; it borrows it. Delay intake to smooth the repayment curve. - ✓
Burnout is often a timing error, not a depletion error.
Synthesis Matrix: Protocol Comparison
| Variable | Morning Protocol | Evening Protocol | Biological Goal |
|---|---|---|---|
| Light Exposure | Maximize Sunlight / 10k Lux |
Minimize Red hue / Dim |
SCN Entrainment |
| Nutrition | Hydration + Tyrosine | Carbohydrates (Starch) | Glucose/Cortisol Balance |
| Physiology | Exercise / Movement | Physiological Sigh / NSDR | Autonomic State Shift |
| Supplementation | Salt / Electrolytes | Ashwagandha / Apigenin | Hormonal Modulation |
Cortisol Rhythm Guide for Energy

Frequently Asked Questions
Does grapefruit juice actually affect cortisol?
Yes. Grapefruit inhibits the CYP3A4 enzyme, which metabolizes cortisol. This extends the half-life of cortisol in the blood. It is a tool for prolongation, not production, but interacts with many medications.
I work night shifts. How do I apply this?
You must invert the lighting protocol relative to your wake time, not the sun. Blast bright light immediately upon your “morning” (waking for the shift) and block all light with blackout curtains/mask during your “night” (daytime sleep).
Why avoid cold showers in the evening?
Cold exposure triggers norepinephrine and cortisol release. While excellent for morning alertness, it is counterproductive to the evening goal of lowering autonomic arousal.
Is ashwagandha safe for daily use?
It is effective for lowering cortisol (11-29% reduction). However, it should be cycled (e.g., 2 weeks on, 1 week off) to prevent receptor downregulation or emotional blunting.
What is the “Physiological Sigh”?
It is a breathing pattern: two inhales through the nose (one long, one short to pop alveoli open) followed by a long, extended exhale through the mouth. It is the fastest mechanical way to reduce heart rate.