Type 2 diabetes is defined by a dual defect: peripheral insulin resistance and progressive pancreatic beta-cell dysfunction. Effective glycemic control requires therapeutic agents that target specific points within the glucose regulation axis. This analysis delineates the five fundamental mechanistic strategies utilized in modern pharmacotherapy.
Contents
Physiological Targets: The Glucose Axis
Homeostasis relies on the interplay between insulin (anabolic, storage) and glucagon (catabolic, release). In type 2 diabetes, this balance is disrupted. The body’s tissues fail to respond to insulin, and the liver inappropriately releases glucose. Pharmacological intervention aims to restore this balance by manipulating supply, demand, or excretion.
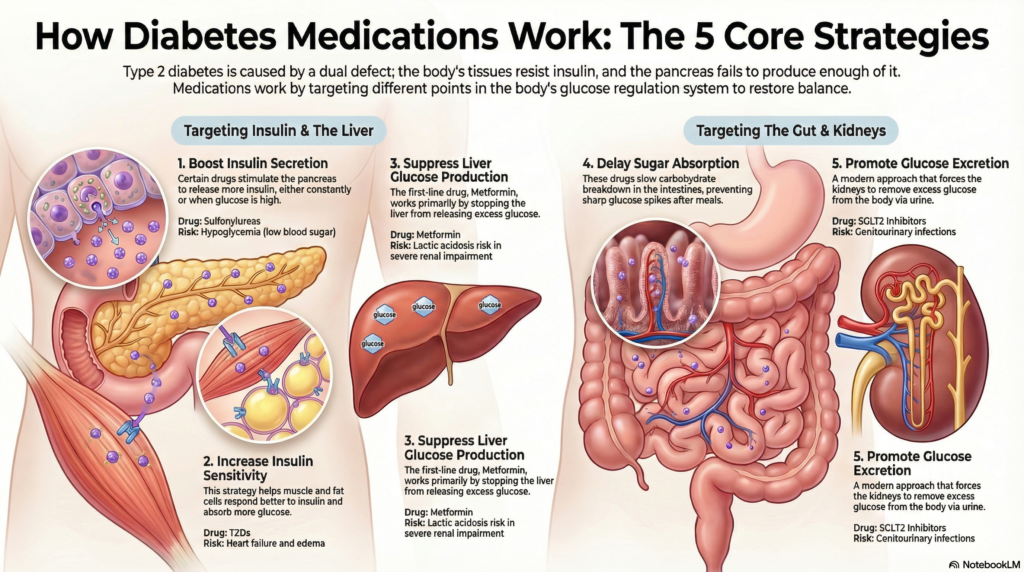
Mechanistic Analysis: The 5 Strategies
We classify antihyperglycemic agents based on their primary physiological lever.
Pharmacodynamic Flow: Strategy 1 (Secretion)
GLP-1 Agonists enhance incretin effect.
1. Enhancing Insulin Secretion
This strategy addresses beta-cell dysfunction or relative insulinopenia.
Sulfonylureas & Meglitinides: Force insulin release independent of glucose levels, carrying a risk of hypoglycemia and weight gain.
Incretin Modulators (GLP-1 RAs & DPP-4 Inhibitors): GLP-1 agonists mimic natural hormones to boost insulin only when glucose is high, while slowing gastric emptying. DPP-4 inhibitors prevent the breakdown of endogenous incretins.
2. Increasing Peripheral Sensitivity
Targeting the “demand” side, Thiazolidinediones (TZDs) act as PPAR-gamma agonists. They enhance glucose uptake in muscle and adipose tissue. While effective for resistance, they are limited by adverse effects including edema, heart failure risks, and bone fractures.
3. Suppressing Hepatic Glucose Output
Metformin (Biguanides) remains the first-line therapy. Its primary mechanism is the inhibition of hepatic gluconeogenesis (production of new glucose). It does not stimulate insulin secretion, making hypoglycemia rare, though gastrointestinal side effects are common.
4. Delaying Carbohydrate Absorption
Alpha-glucosidase inhibitors target the intestinal lumen. By inhibiting enzymes responsible for carbohydrate breakdown, they blunt postprandial hyperglycemic peaks. Their utility is often limited by significant gastrointestinal intolerance.
5. Promoting Renal Excretion
SGLT2 Inhibitors represent a shift from hormonal modulation to hemodynamic filtration. By blocking glucose reabsorption in the proximal renal tubule, they induce glycosuria (excreting sugar in urine). This mechanism operates independently of insulin.
Applied Clinical Approach: The Dr. Belh Framework
1. Observation
Identify the dominant phenotype. Is the patient insulin resistant (high visceral fat) or insulin deficient (lean, sarcopenic)?
2. Context
Assess comorbidities. For patients with heart failure or CKD, SGLT2 inhibitors are prioritized regardless of HbA1c.
3. Solution
Combine mechanisms. Do not layer two drugs affecting the same pathway. Mix sensitivity (Metformin) with excretion (SGLT2).
Therapeutic Intensification Timeline
(SGLT2 or GLP-1)
or Insulin Initiation
Key Clinical Takeaways
- Hypoglycemia Risk: Highest with Sulfonylureas and Insulin; negligible with Metformin, SGLT2i, and GLP-1 RAs.
- Weight Impact: GLP-1 RAs and SGLT2i promote weight loss; Sulfonylureas and TZDs may cause weight gain.
- Renal Protection: SGLT2 inhibitors effectively reduce progression of diabetic kidney disease.
- Contraindication: Metformin must be avoided in unstable heart failure or severe renal impairment due to lactic acidosis risk.
Synthesis: Mechanistic Comparison
| Strategy | Drug Class | Mechanism | Key Concern |
|---|---|---|---|
| Secretion | Sulfonylureas | Stimulate Beta-cells | Hypoglycemia |
| Secretion | GLP-1 RA | Incretin Mimetic | GI Distress |
| Sensitivity | TZDs | PPAR-gamma Agonist | Heart Failure |
| Output | Metformin | Inhibit Gluconeogenesis | Lactic Acidosis |
| Excretion | SGLT2i | Block Glucose Reuptake | Infection |
Clinical FAQ
Why does Metformin not cause hypoglycemia?
Metformin inhibits hepatic glucose production but does not stimulate insulin secretion. Therefore, even in the absence of glucose intake, it does not drive blood sugar below physiological baselines.
What is the primary advantage of SGLT2 inhibitors beyond glucose control?
They offer significant cardiovascular and renal protection, reducing the risk of hospitalization for heart failure and slowing the progression of chronic kidney disease.
Why are Sulfonylureas often considered second-line despite high efficacy?
They are associated with weight gain and a high risk of hypoglycemia. Furthermore, there is concern regarding faster exhaustion of remaining beta-cell function compared to other agents.
How do GLP-1 Agonists aid in weight loss?
They delay gastric emptying (increasing satiety) and act centrally on the hypothalamus to reduce appetite, leading to reduced caloric intake.
Are these strategies used in Type 1 Diabetes?
Generally, no. Type 1 Diabetes is characterized by absolute insulin deficiency. While some agents (like SGLT2i) have been studied as adjuncts, insulin remains the mandatory life-sustaining therapy.