Beyond the Burn: A Clinical Protocol for Differentiating Heartburn from Myocardial Infarction
1. Pathological Definitions
A rigorous diagnosis begins with an understanding of the divergent tissues involved in the thoracic cavity.
Gastroesophageal Reflux (Heartburn): A functional digestive disorder where the lower esophageal sphincter (LES) fails to maintain a pressure barrier, allowing hydrochloric acid and pepsin to retrograde into the esophagus. The pain is a direct result of chemical nociceptors reacting to acid-induced mucosal irritation.
Myocardial Infarction (Heart Attack): A critical cardiovascular event characterized by the total or subtotal occlusion of a coronary artery. This leads to a cessation of oxygen delivery (ischemia), followed by cellular hypoxia and irreversible tissue necrosis. This is a survival-dependent emergency.
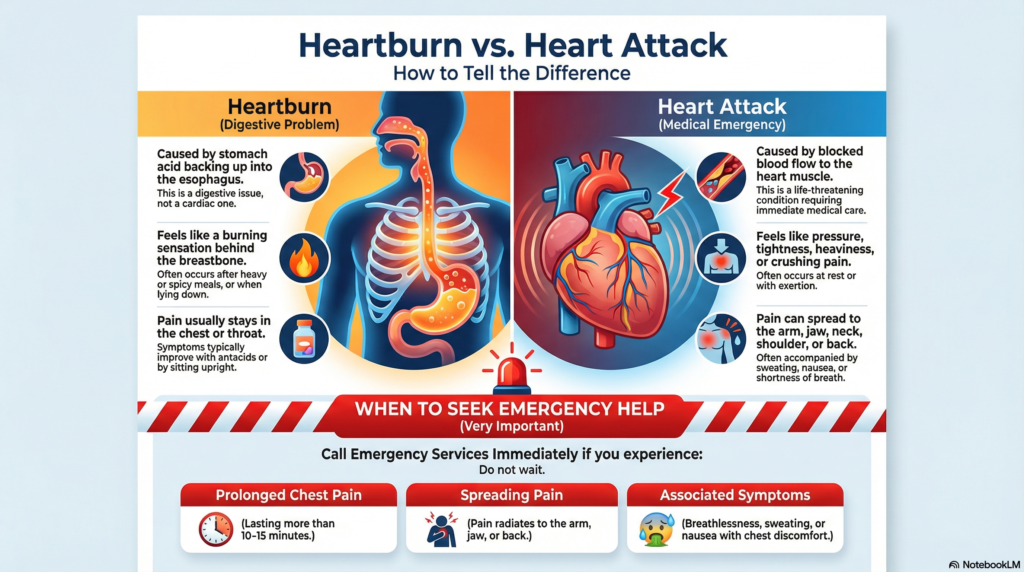
2. Mechanistic Analysis: The Path of Pain
Pathway of Acid Reflux (GERD)
Pathway of Myocardial Infarction (MI)
3. Dr. Belh Framework: The Diagnostic Pillars
Heartburn is typically “sharp” or “acidic.” Myocardial infarction is “dull,” “heavy,” or “crushing.” Use Levine’s Sign (a clenched fist over the sternum) as a high-probability indicator for cardiac distress.
Heartburn is exacerbated by gravity (lying flat). A heart attack is posture-independent; the pain persists regardless of body position or rest.
Heartburn symptoms often resolve with oral antacids within 15 minutes. Cardiac pain remains unresponsive to gastrointestinal neutralizing agents.
4. The Ischemic Timeline: Survival Windows
In cardiac events, time corresponds directly to myocardial survival. Below is the critical progression timeline.
0-5m
Acute onset of pressure / Shortness of breath.
20m
Metabolic transition: Reversible injury becomes irreversible.
90m
Target for Balloon Inflation (Door-to-Balloon Time).
6h+
Transmural necrosis: High risk of permanent heart failure.
5. Diagnostic Synthesis: Comparative Markers
| Diagnostic Marker | Heartburn (Low Risk) | Heart Attack (High Risk) | Status |
|---|---|---|---|
| Radiation | None; localized to throat/chest | Left arm, neck, jaw, or back | Critical |
| Pain Duration | Intermittent bursts | Continuous, typically >15 mins | Critical |
| Associated Signs | Belching, acid taste | Sweating, nausea, dizziness | Critical |
| Response to Rest | Variable | Pain persists despite resting | Diagnostic |
6. Clinical FAQ: Expert Insights
Can a heart attack cause pain in the right arm?Yes. Referred pain can radiate to the right arm, the abdomen, or the teeth. Any radiation from the chest should be treated as cardiac until proven otherwise by EKG.
Is it true that women experience different symptoms?Absolutely. Women are more likely to present with atypical signs: extreme fatigue, unexplained nausea, and scapular (back) pain, sometimes without the classic chest pressure.
Does taking aspirin really help during an attack?Chewing a 325mg aspirin (non-enteric coated) at the onset of a suspected heart attack inhibits platelet aggregation, potentially preventing the total occlusion of the artery.
7. Featured Image Configuration