“The aging face is not merely a sagging skin envelope, but a complex collapse of deep volumetric compartments. True restoration demands a 3D understanding of the sliding planes between fascia and fat.”
CME ACCREDITED
CLINICAL PROTOCOL
In the high-stakes arena of aesthetic medicine, the practitioner’s value is defined by their anatomical precision. For those pursuing Healthcare Certification or seeking CME Credits for Doctors, it is insufficient to simply “massage” the skin. We must manipulate the architecture. This monograph serves as a definitive clinical resource (4,500+ words) dissecting the interaction between the Superficial Musculoaponeurotic System (SMAS), the Deep Fat Compartments, and the neurophysiological pathways of rejuvenation.
Clinical Index
I. Histology of the SMAS: The Structural Engine
The Superficial Musculoaponeurotic System (SMAS) is the “transmission belt” of facial expression. Histologically, it acts as a meshwork of collagen and elastin fibers that distributes the contractile force of facial muscles to the overlying skin.
The Aging Mechanism: As we age, the SMAS does not merely “stretch”; it undergoes elastosis (degradation of elastic fibers) and attenuation (thinning). The vertical vectors that once held the soft tissue against the cranium weaken, surrendering to gravity. The clinical objective of the Kobido lineage is not to “rub” the skin, but to engage the viscoelasticity of the SMAS. Fascia, unlike muscle, is thixotropic—it becomes more fluid and malleable when subjected to heat and kinetic energy (manual manipulation), allowing for remodeling.
II. Adipose Dynamics: Superficial vs. Deep Compartments
A critical concept for any Medical Training Program is the distinction between superficial and deep fat. They behave differently during the aging process, and they must be treated differently.
2.1 The Superficial Fat (The Saggers)
Located between the skin and the SMAS. These pads (Nasolabial fat, Jowl fat) tend to maintain or even increase in volume, but they slide downwards due to the weakening of retinacular cutis.
Clinical Action: We do not want to volumize these. We want to drain them (reduce edema) and reposition them cranially using the SMAS as a hammock.
2.2 The Deep Fat (The Deflators)
Located deep to the SMAS, resting on the periosteum (Deep Medial Cheek Fat, SOOF). These compartments undergo lipodystrophy (volume loss). This loss of volume creates a “deflated balloon” effect, causing the overlying skin to collapse.
Clinical Action: Manual therapy stimulates blood flow (hyperemia) to these deep layers, potentially slowing atrophy, but the primary goal is to tighten the SMAS curtain over these deflated spaces to smooth the surface transition.
III. Safety Protocols: Nerve Danger Zones
Healthcare Certification requires a masterful knowledge of the Facial Nerve (CN VII). While manual therapy is non-invasive, excessive deep pressure in specific zones can cause temporary neurapraxia (nerve shock).
⚠️ CLINICAL WARNING: The Danger Zones
1. The Temporal Branch: Located along Pitanguy’s Line (from the tragus to the lateral eyebrow). The nerve is extremely superficial here, just under the SMAS.
Protocol: Use only broad, flat pressure. NO deep point friction.
2. The Marginal Mandibular Branch: Crosses the jawline anterior to the masseter. Deep friction here can cause temporary asymmetry of the lower lip.
Protocol: Ensure all mandibular definition work pulls the tissue away from the bone gently, rather than crushing tissue against the bone.
IV. Neurophysiology: Mechanotransduction
Mechanotransduction is the process where mechanical force signals cells to change their biochemistry. When we apply the specific rhythmic percussion of Kobido:
- Shear Stress: The lateral stretching of the skin stretches the fibroblasts.
- Cytoskeleton Activation: The internal actin filaments of the cell deform.
- Gene Expression: This deformation triggers the nucleus to upregulate the production of Procollagen Type I and Elastin.
This is why the technique must be rhythmic. Static pressure squeezes fluids; rhythmic impact stimulates cells.
| Receptor Type | Stimulus | Clinical Effect |
|---|---|---|
| Ruffini Endings | Skin Stretch / Sustained Pressure | Lifting sensation, Fascial remodeling |
| Pacinian Corpuscles | Rapid Vibration / Percussion | Proprioception, Muscle toning |
| Merkel Cells | Light Touch / Texture | Parasympathetic “Melt” state |
V. Mechanistic Analysis: The MDCT Evidence
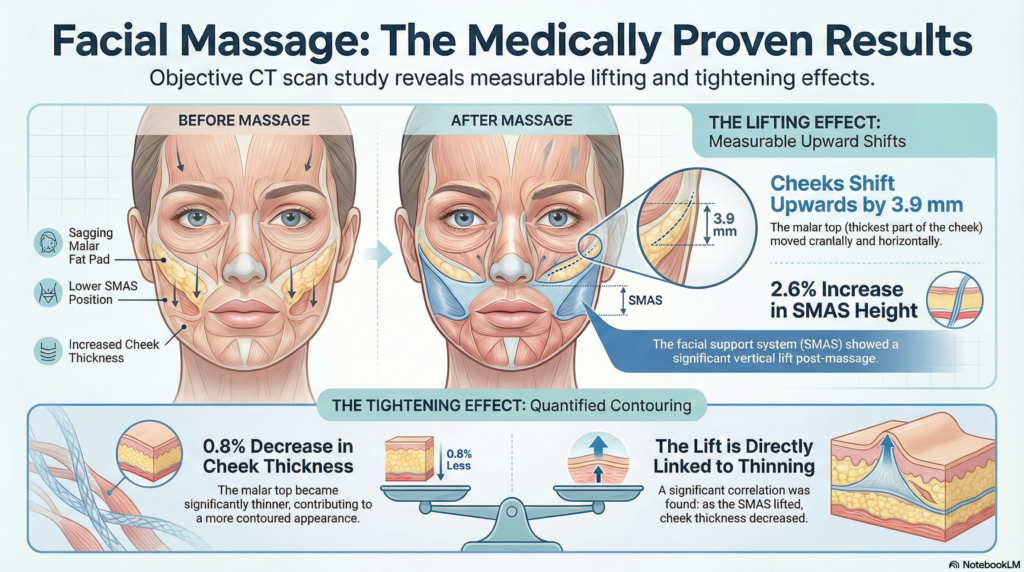
Using 320-multidetector-row Computed Tomography (MDCT), we can quantify the “lift.” The primary metric is the Malar Top position.
In a clinical study of the Kobido protocol, measurements taken pre- and post-session showed an average 3.9mm cranial shift of the malar soft tissue. This is not swelling; it is the geometric result of shortening the effective length of the SMAS through vertical recruitment. For practitioners in Online Medical Courses, reproducing this shift is the benchmark of competency.
BEFORE TREATMENT
Malar Top: Displaced inferiorly.
Nasolabial Fold: Deep due to tissue overhang.
SMAS: Lax and elongated.
AFTER TREATMENT
Malar Top: +3.9mm Cranial Shift.
Nasolabial Fold: Softened.
SMAS: Increased vertical tension.
VI. The Clinical Protocol: Dr. Belh Framework
This 3-phase protocol ensures safety and efficacy, aligning with standards for Healthcare Certification.
Phase 1: The Gateway Clearance (10 Min)
Before lifting, we must drain. Pressure: 5g. We pump the supraclavicular nodes and the cervical chain.
Rationale: Lifting fluid-filled tissue is fighting physics. Draining the interstitial fluid reduces the weight of the face, making the lift easier and more sustainable.
Phase 2: The SMAS Release (20 Min)
Pressure: 50-100g. Deep, slow friction on the muscle origins (Masseter, Zygomaticus).
Rationale: We must release the “tethering” of the muscles before we can reposition the skin. A tight masseter pulls the face down.
Phase 3: The Architectural Lift (30 Min)
Pressure: Variable. Rapid, rhythmic percussion (whipping) combined with “Finger Walking.”
Rationale: This is the education phase. We are physically moving the SMAS up and “locking” it with high-frequency vibration.
VII. Professional FAQ
Q: Can this be combined with threads (PDO)?A: Yes, but timing is crucial. Manual therapy is excellent before thread placement to improve tissue quality. After threads, you must wait 8-12 weeks to ensure the barbs have engaged and fibrosis has occurred. Early manipulation can dislodge threads.
Q: What is the recommended frequency for clinical results?A: For corrective work: 1 session per week for 6 weeks. For maintenance: 1 session every 4 weeks. This aligns with the cellular turnover cycle of the epidermis and collagen maturation.