Sleep fragmentation is frequently misdiagnosed as benign fatigue or simple snoring, masking a critical respiratory failure. Obstructive Sleep Apnea (OSA) constitutes a mechanical blockade of the airway, resulting in intermittent hypoxia and cardiovascular strain. This analysis examines the anatomical etiology, systemic consequences, and therapeutic protocols for OSA.
1. Pathophysiology: Defining the Blockade
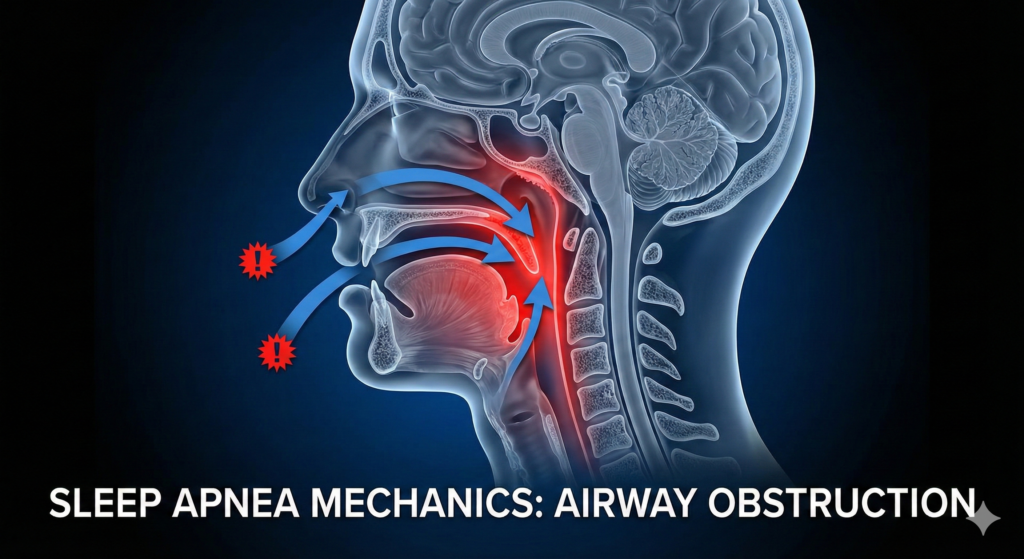
Obstructive Sleep Apnea is not a neurological failure of respiratory drive; it is an anatomical obstruction. In a healthy upper airway, pharyngeal muscle tone maintains patency against the negative pressure generated during inhalation. In OSA pathology, this muscular tone is insufficient.
During REM and non-REM sleep, the relaxation of the genioglossus (tongue) and soft palate allows these structures to collapse posteriorly against the pharyngeal wall. This creates a physical seal, causing a complete cessation of airflow (apnea) despite continued respiratory effort. The result is a cycle of hypoxia and sympathetic nervous system activation that precludes restorative sleep stages.
2. Mechanistic Analysis: The Hypoxic Loop
The progression from sleep onset to apneic event follows a predictable biomechanical sequence. Understanding this causality is essential for recognizing the severity of the condition beyond the audible symptom of snoring.
The Apnea-Arousal Cascade
1. Muscular Relaxation
2. Negative Pressure Collapse
3. Systemic Hypoxia
4. Cortical Micro-Arousal
3. Dr. Belh Framework: The Clinical Approach
To effectively manage OSA, we apply a tripartite framework: precise observation of symptoms, contextualization of anatomical risk, and targeted mechanical intervention.
1. Observation
The patient rarely reports the apnea itself. Look for secondary indicators: morning headaches (vasodilation), excessive daytime sleepiness (EDS), and partner-reported gasping. The absence of recall does not indicate the absence of pathology.
2. Context
OSA is multifactorial. While obesity (adipose tissue in the pharynx) is a primary driver, anatomical factors such as retrognathia (recessed jaw) and age-related loss of pharyngeal muscle tension are critical non-weight related contributors.
3. Solution
Treatment requires physical maintenance of the airway. CPAP (pneumatic splinting) is the gold standard. Mandibular Advancement Devices (MAD) offer mechanical alternatives for mild cases by protruding the jaw to anteriorly displace the tongue.
4. The Nightly Cycle: A Temporal Analysis
The impact of OSA is cumulative. A single event lasts seconds, but the repetition creates a fragmented sleep architecture. The following timeline illustrates the cyclical nature of a single apneic episode.
5. Clinical Extraction Zone
- Silent Hypoxia: Patients may experience hundreds of micro-awakenings per night without conscious memory, manifesting solely as daytime cognitive deficit.
- Cardiovascular Load: The repeated adrenergic surges required to re-initiate breathing significantly increase the risk of hypertension, arrhythmia, and stroke.
- Anatomical Variety: Risk is not limited to obesity; retrognathia, tonsillar hypertrophy, and soft palate morphology are key structural determinants.
- Therapeutic Efficacy: CPAP therapy is highly effective, mechanically acting as a pneumatic splint to prevent pharyngeal collapse.
6. Synthesis: Untreated vs. Treated Profiles
The following data delineates the physiological divergence between a patient with untreated OSA and one managing the condition via CPAP or oral appliances.
| Parameter | Untreated OSA | Therapeutic Outcome |
|---|---|---|
| Sleep Architecture | Fragmented; No Deep Sleep | Consolidated; Restorative REM |
| Blood Oxygen | Intermittent Hypoxia (SpO2 drops) | Stable Saturation (>95%) |
| Cardiovascular Status | Hypertensive; High Stress Load | Normotensive; Reduced Strain |
| Daytime Function | Chronic Fatigue, Irritability | Alertness, Emotional Stability |
7. Featured Image Specification
8. Frequently Asked Questions
Can thin people get sleep apnea?
Yes. While weight is a factor, anatomical features like a recessed chin, large tonsils, or a naturally narrow airway can cause OSA in individuals with low BMI.
Is snoring always a sign of apnea?
No, but loud, irregular snoring accompanied by gasping or silence (cessation of breathing) is a strong clinical indicator of OSA.
Can OSA be cured permanently?
OSA is typically a chronic condition requiring management (CPAP, oral appliances). Surgical options exist but success rates vary based on specific anatomy.
Why do I wake up with a headache?
Morning headaches in OSA are often caused by vasodilation resulting from carbon dioxide retention and oxygen deprivation during sleep.
Is CPAP the only option?
While CPAP is the gold standard for severe cases, mild to moderate OSA can often be treated effectively with custom-fitted mandibular advancement devices (dental appliances).