1. Clinical Definition and Neurobiological Substrate
Bipolar disorder (formerly manic-depressive illness) is a chronic, episodic mood disorder. Pathophysiologically, it involves a complex interplay of genetic vulnerability and environmental stressors, leading to dysregulation in the dopaminergic and serotonergic pathways. Unlike unipolar depression, the defining feature of bipolar disorder is the presence of at least one episode of mania or hypomania.
The “pendulum” analogy, often used in patient education, describes the oscillation between two distinct poles:
- The Manic Pole: Characterized by hyperarousal, increased goal-directed activity, and reduced need for sleep.
- The Depressive Pole: Characterized by psychomotor retardation, anhedonia, and cognitive impairment.
- Euthymia: The “baseline” mood state between episodes, though sub-syndromal symptoms often persist.
For professionals seeking CME credits for doctors, understanding the nuance of these shifts is critical for accurate diagnosis and preventing iatrogenic harm (e.g., antidepressant-induced mania).
2. Mechanistic Analysis: The Pathophysiology of Mood Swings
The progression of a bipolar episode follows a recognizable trajectory. We can visualize the mechanism of action through the following flow structure, moving from biological predisposition to the manifestation of acute symptoms.
Figure 1: The “Kindling” Progression Model
(Heritability > 80%, HPA Axis dysregulation)
(Circadian rhythm disruption, Substance use)
(Dopamine hypersensitivity = Mania / Depletion = Depression)
(Cognitive sequelae, increased susceptibility to future episodes)
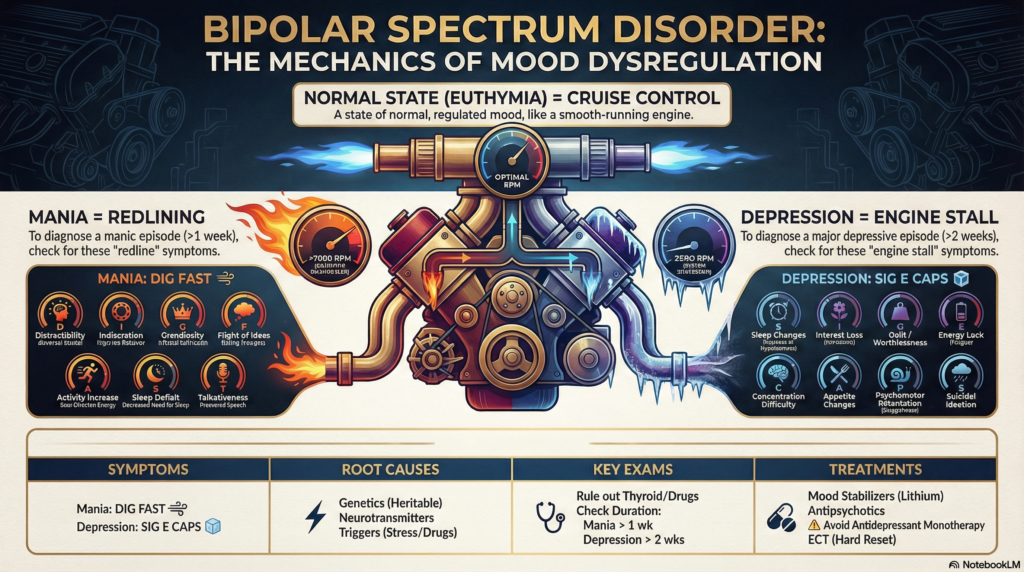
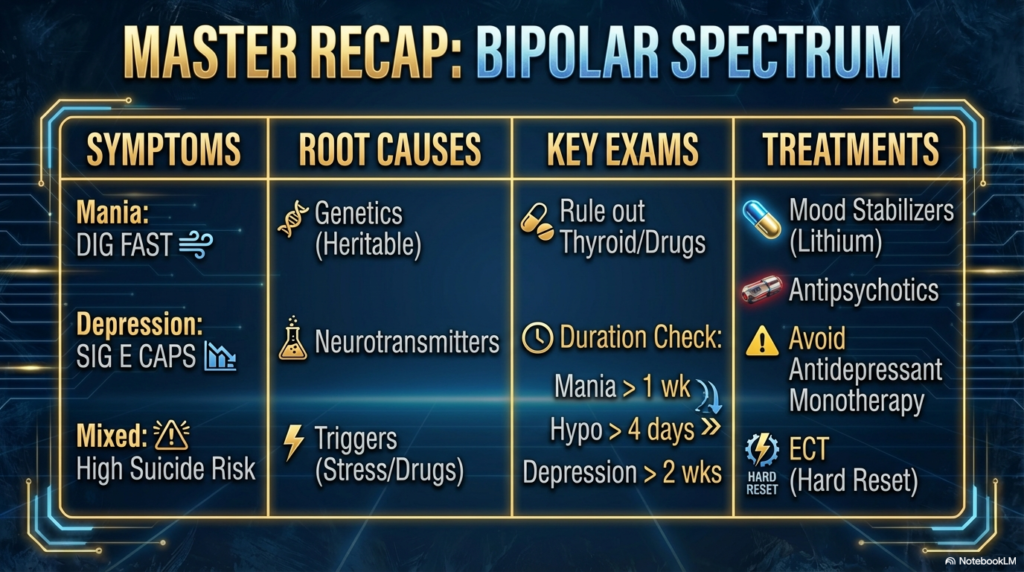
The Mania Spectrum: D.I.G.F.A.S.T.
To standardize the identification of mania in Medical Training Programs, the mnemonic D.I.G.F.A.S.T. is the gold standard. A diagnosis of mania requires elevated mood plus 3 of these symptoms (or 4 if the mood is only irritable).
- Distractibility: Attention is pulled by irrelevant external stimuli.
- Indiscretion (Guilt-free high-risk behavior): Spending sprees, sexual promiscuity, reckless driving. The prefrontal cortex’s inhibitory control is compromised.
- Grandiosity: Inflated self-esteem ranging from unshakeable confidence to delusional omnipotence.
- Flight of Ideas: Subjective experience of racing thoughts; manifested as pressured speech.
- Activity Increase: Excessive planning and participation in multiple activities (goal-directed) or psychomotor agitation (non-goal-directed).
- Sleep Deficit: A distinguishing marker from insomnia. The patient sleeps 2-3 hours but feels fully rested.
- Talkativeness: Pressured speech that is difficult to interrupt.
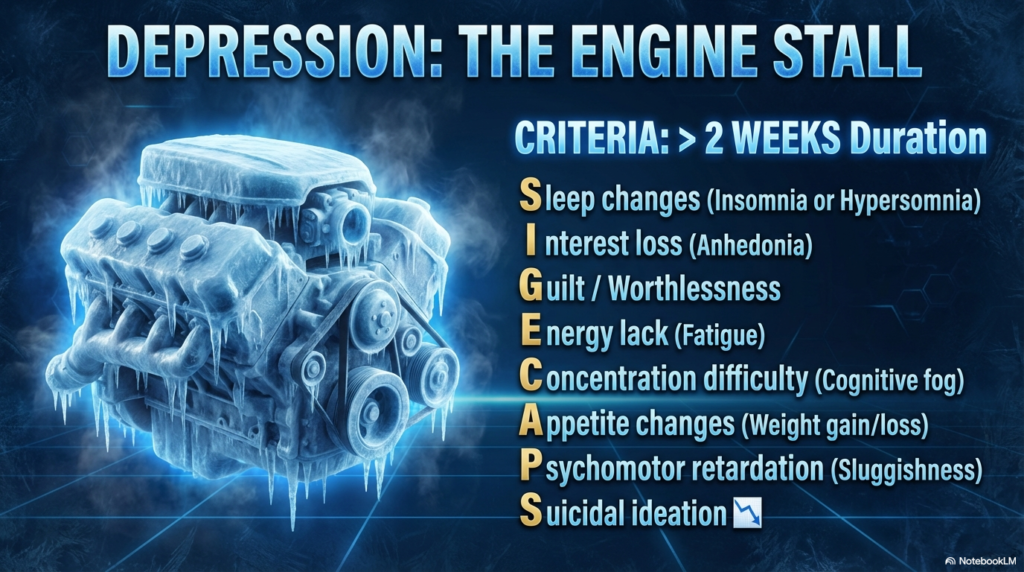
The Depressive Anchor: The Cognitive Trap
While mania is the defining feature, depression is the predominant state of the illness. Bipolar depression is often termed a “heavy anchor” because of its distinct quality of psychomotor retardation (sluggishness) compared to the often agitated nature of unipolar depression. The “Cognitive Trap” refers to the patient’s rumination on past failures, creating a feedback loop of worthlessness that complicates therapeutic intervention.
3. Applied Approach: The Dr. Belh Framework
Effective management requires moving beyond symptom checklists to a holistic operational framework. In my clinical experience and healthcare certification courses, I advocate for the “Observation-Context-Solution” triad.
Principle 1: Observation
Quantify the Subjective. Patients cannot rely on “feeling.” We must use mood charting apps or journals to track sleep hours and irritability ratings. Data beats perception.
Principle 2: Context
Respect the Rhythm. Bipolar is a circadian disorder. Treatment is not just medication; it is the rigid enforcement of sleep/wake cycles and social rhythms (IPSRT).
Principle 3: Solution
Layered Defense. Monotherapy is rarely sufficient. We combine mood stabilizers (the floor) with antipsychotics (the ceiling) and CBT (the walls) for stability.
4. Differential Diagnosis and Classification
Accurate sub-typing dictates prognosis and pharmacotherapy. The table below synthesizes the key differentiators between Bipolar I, II, and Cyclothymia.
| Feature | Bipolar I Disorder | Bipolar II Disorder | Cyclothymic Disorder |
|---|---|---|---|
| Manic Episode | Required (Full Mania) | Absent | Absent |
| Hypomania | Common, but not required | Required (>4 Days) | Frequent (Sub-threshold) |
| Depression | Common, but not required | Required (MDD) | Frequent (Sub-threshold) |
| Psychosis | Possible during Mania | Absent (in hypomania) | Absent |
| Functional Impact | Marked impairment; often hospitalization | Change in functioning; observable by others | Distress or impairment |
5. The Treatment Arc: A Chronological Perspective
Recovery is not an event; it is a process. The following timeline illustrates the typical phases of treatment for a patient presenting with an acute manic episode. Adherence to this timeline is emphasized in all accredited online medical courses on psychiatry.
Acute Phase
Weeks 0-8
Safety, Stabilization, Aggressive Pharmacotherapy (Antipsychotics/Lithium).
Continuation
Months 2-6
Relapse prevention, Titration of meds, Introduction of Psychotherapy.
Maintenance
6 Months +
Lifestyle management, Monitoring for metabolic side effects, Social reintegration.
6. Key Clinical Takeaways
- Paradox of Mania: Patients often resist treatment during mania because the symptoms feel “good” or “powerful” compared to their baseline.
- Diagnostic Precision: Bipolar II is frequently misdiagnosed as Unipolar Depression; screen for history of hypomania in all depressed patients.
- Pharmacology: Lithium remains the gold standard for suicide prevention in bipolar populations.
- Education: Psychoeducation for the family is as effective as medication adherence in reducing hospitalization rates.
7. Bipolar Disorder: Clinical Mechanisms, Diagnosis, and Management Strategies
8. Frequently Asked Questions
Q: What is the most common age of onset?
A: The peak age of onset is between 15 and 25 years old. Late-onset bipolar (after 50) should trigger a workup for neurological causes.
Q: Can Bipolar Disorder be cured?
A: No, it is a chronic, lifelong condition. However, with consistent medication and lifestyle management, patients can achieve long periods of euthymia (stability).
Q: Are there online medical courses for specific bipolar therapies?
A: Yes, many institutions offer specialized training in Interpersonal and Social Rhythm Therapy (IPSRT) and CBT for Bipolar Disorder.
Q: Is heredity the only cause?
A: While genetics play a massive role (80-90% heritability), environmental stressors, drug use, and sleep disruption are critical triggers for gene expression.
Q: How does Bipolar II differ from moodiness?
A: Bipolar II involves distinct episodes of hypomania lasting at least 4 days and major depression lasting 2 weeks. Standard moodiness is transient and reactive to events.