The High-Yield Endocrine Mnemonic Handbook: PANCE & Board Essentials
Endocrine pathology follows a strict logic of feedback loops and laboratory thresholds. Mastering this forest of shifting hormones requires structural anchors rather than rote memorization. This guide provides the clinical “navigational map” for rapid board-certified recall.
1. Definition: The Clinical Endocrine Scope
Endocrine Board Mastery is defined as the cognitive ability to identify the precise failure point in a chemical signaling pathway. It involves distinguishing between Primary (target gland), Secondary (pituitary), and Tertiary (hypothalamus) pathologies. In the clinical board context, success depends on correctly interpreting laboratory values—often referred to as the “Gold Standard” criteria—which serve as the definitive pillars of patient diagnosis and board-level precision.
2. Mechanistic Analysis: The Hierarchy of Control
Mechanistically, most endocrine disorders arise from either production failure or receptor resistance. When analyzing a case, the relationship between the stimulus (Tropic hormone) and the output (End hormone) is the critical diagnostic link. If the End hormone is low while the Tropic hormone is high, the gland itself is the failure point (Primary dysfunction). Conversely, if both are low, the control center (Pituitary/Hypothalamus) has failed (Secondary/Tertiary dysfunction).
Primary Failure
Secondary Failure
3. The Dr. Belh Framework (A-C-S)
To process board prompts efficiently, apply this three-tier logic to every clinical scenario:
1. Observation
Identify the physical hallmark: Exophthalmos, Hyperpigmentation, or Truncular Obesity.
2. Context
Verify current lab thresholds. Is the A1C above $\ge 6.5\%$? Is the GFR stable for drug initiation?
3. Solution
Execute the sequence: Alpha-blockade before Beta-blockade; Fluids before Insulin.
4. Diabetes Diagnostic Pillar
A diagnosis of Diabetes Mellitus requires strict adherence to quantitative data. If results are discordant (e.g., A1C is borderline but Glucose is high), the 2-hour Glucose Tolerance Test (GTT) serves as the gold standard arbitrator.
| Modality | Diagnostic Threshold | Indicator |
|---|---|---|
| Fasting Glucose | $\ge 126$ mg/dL | POSITIVE |
| Hemoglobin A1C | $\ge 6.5\%$ | POSITIVE |
| 2-Hour GTT | $\ge 200$ mg/dL | GOLD STANDARD |
5. Medication Memory Palace: Safety & Weight
When studying DM pharmacology, the boards prioritize Weight Dynamics and Contraindications. Use the following mnemonics to differentiate between agents:
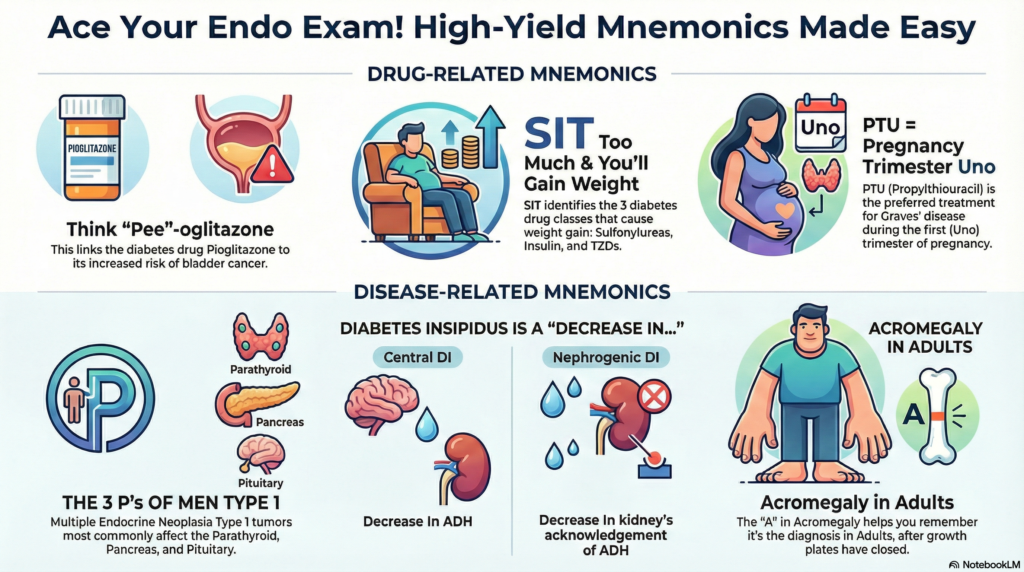
- The “SIT” Rule (Weight Gain): If you SIT too much, you gain weight. Use this for Sulfonylureas, Insulin, and Thiazolidinediones.
- GL-I-FROZEN (SGLT2): For drugs ending in -gliflozin. Glucose Is “FROZEN” out of the body through the urine. They are weight-neutral and heart-protective.
- The Pioglitazone “P” Connection: Associate the “P” in Pioglitazone with Pee (increased bladder cancer risk).
6. Thyroid & Parathyroid Precision
Thyroid management shifts dramatically during pregnancy. The timing of drug administration is vital to fetal safety.
(Trimester “Uno”)
(Lower toxicity risk)
Breastfeeding safety
7. Emergency Endocrine: DKA & Crisis
When endocrine systems reach their breaking point, the priority is stabilization over hormonal correction. In Diabetic Ketoacidosis (DKA), the management must follow this strict sequence to avoid fatal outcomes like cerebral edema or cardiac arrhythmia:
- Priority #1: IV Fluids (Isotonic Saline). Patients are volume-depleted; rehydration must precede all else.
- Priority #2: Check Potassium ($K^+$). If $K^+ < 3.3$, hold insulin and replace potassium first.
- Priority #3: Insulin Infusion. Only after volume expansion and K+ stabilization.
High-Yield Extraction Zone (Key Points)
- Pheochromocytoma: Never give Beta-blockers first. Use Alpha-blocker then Beta-blocker (Order of the Alphabet).
- MEN1 Syndrome: The 3 Ps (Parathyroid, Pancreas, Pituitary).
- Metformin: Hold for 48 hours before/after IV contrast to prevent Lactic Acidosis.
- Acromegaly: Starts with “A” for Adults (post-epiphyseal closure).
- Chvostek’s Sign: Elicited by tapping facial nerve; indicates Hypocalcemia.
50 High Yield Endocrine Questions for Exam Mastery
8. Endocrine Board FAQ
Q1: What is the most common cause of hypothyroidism in the US?
A: Hashimoto’s Thyroiditis.
Q2: Why must Alpha-blockers be given before Beta-blockers in Pheochromocytoma?
A: To prevent unopposed alpha-mediated vasoconstriction, which causes a hypertensive crisis.
Q3: What is the most common type of thyroid cancer?
A: Papillary Carcinoma (remember “P” for Popular).
Q4: What electrolyte abnormality is hallmark for Addison’s Disease?
A: Hyponatremia and Hyperkalemia (low Aldosterone).
Q5: What drug is used for Central Diabetes Insipidus?
A: Desmopressin (DDAVP).