Systematic Protocol for Cardiovascular Physical Examination: A Hemodynamic Synthesis
Cardiovascular physical examination remains the cornerstone of clinical diagnosis, transforming physical signs into hemodynamic insights. This article delineates a rigorous, head-to-toe interrogation of the body’s structural and circulatory integrity to eliminate diagnostic gaps. By adhering to a standardized protocol, clinicians can synthesize complex findings into a unified pathological profile.
Defining the Cardiovascular Interrogation
The cardiovascular examination is not a checklist of tasks but a systematic interrogation of the body’s hemodynamic status. It involves the integration of sensory data—visual, tactile, and auditory—to evaluate the pump (heart), the pipes (vasculature), and the perfusion (end-organ status).
Mechanistic Analysis: From Signs to Physiology
Clinical signs are peripheral manifestations of central failures. The relationship follows a direct causal chain:
Applied Approach: The Dr. Belh Framework
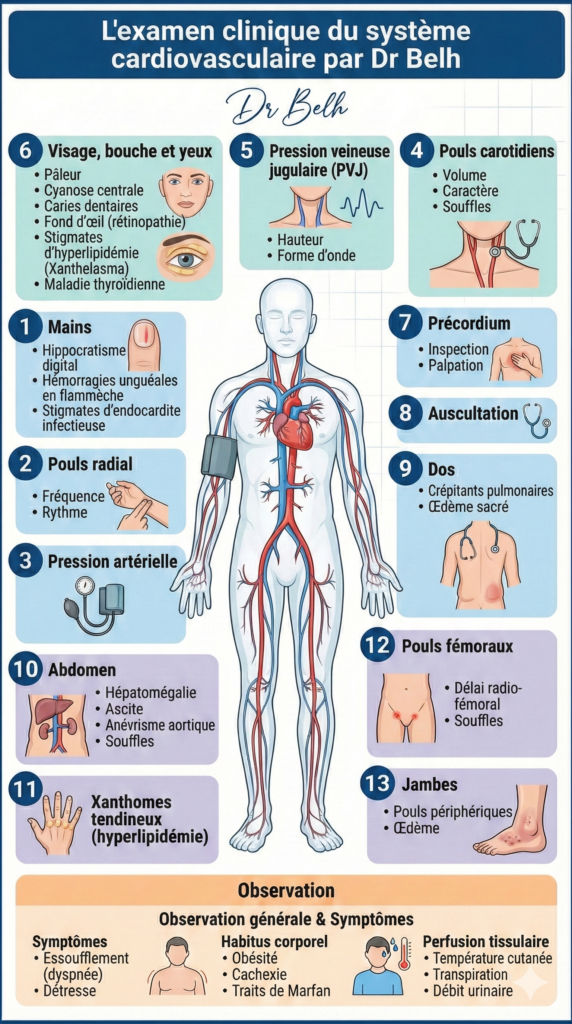
1. ObservationIdentify global hemodynamic cues (habitus, respiratory effort) before patient contact.
2. ContextIntegrate peripheral markers (hands, eyes) with central pressure readings (JVP).
3. SolutionExecute the “Z-pattern” auscultation to confirm structural valvular integrity.
Standardized 6-Step Clinical Protocol
Global Observation
Upper Extremities
Cephalic & Cervical
Precordium Core
Abdominal Status
Lower Extremities
Key Clinical Extraction Points
- JVP Elevation: A vertical height >3cm above the Angle of Louis indicates right-heart congestion.
- Pulsus Tardus: A slow-rising carotid pulse is a specific indicator of significant Aortic Stenosis.
- Atrial Fibrillation: Characterized by an “irregularly irregular” radial rhythm.
- Clubbing: Suggests chronic cyanotic heart disease or infective endocarditis.
Synthesis Table: Peripheral vs. Central Signs
| Clinical Sign | Location | Diagnostic Priority | Result Status |
|---|---|---|---|
| Raised JVP | Neck (Internal Jugular) | Central Pressure | Critical |
| Splinter Hemorrhages | Nail Beds | Infective Index | Caution |
| Normal S1/S2 | Precordium | Valvular Function | Positive |
A Guide to Cardiovascular Examination
Expert FAQ
1. Why is the 45-degree angle critical for JVP?
It optimizes the visualization of the internal jugular vein oscillations relative to the sternal angle.
2. What does a “heave” represent?
A palpable impulse suggesting ventricular hypertrophy, usually the right ventricle.
3. Can peripheral edema occur without heart failure?
Yes, venous insufficiency or renal failure can also cause pitting edema.
4. Why use the bell of the stethoscope?
To detect low-frequency sounds such as the S3 gallop or mitral stenosis rumble.
5. What is radio-femoral delay?
A timing discrepancy between pulses indicating Coarctation of the Aorta.