Time remains the fundamental currency in neuro-emergency medicine. Effective stroke management requires a transition from checklist-based tasks to an integrated clinical protocol. This manual deconstructs the essential diagnostic and therapeutic maneuvers required within the hyper-acute window.
Definition: The Neuro-Vascular Crisis
Acute stroke is a clinical syndrome characterized by a sudden-onset focal neurological deficit resulting from a vascular etiology. Whether ischemic or hemorrhagic, the event triggers a cascade of cellular failure where cerebral blood flow (CBF) drops below critical thresholds, leading to the rapid loss of neuronal integrity.
Mechanistic Analysis: Flow vs. Pressure
The pathophysiology of acute stroke follows a predictable cause-and-effect relationship based on the primary vascular insult:
In ischemic cases, the penumbra—a salvageable zone of brain tissue—is maintained by collateral circulation. If reperfusion is not achieved, this zone inevitably transitions to the infarcted core.
The Dr. Belh Framework: Triple-Phase Approach
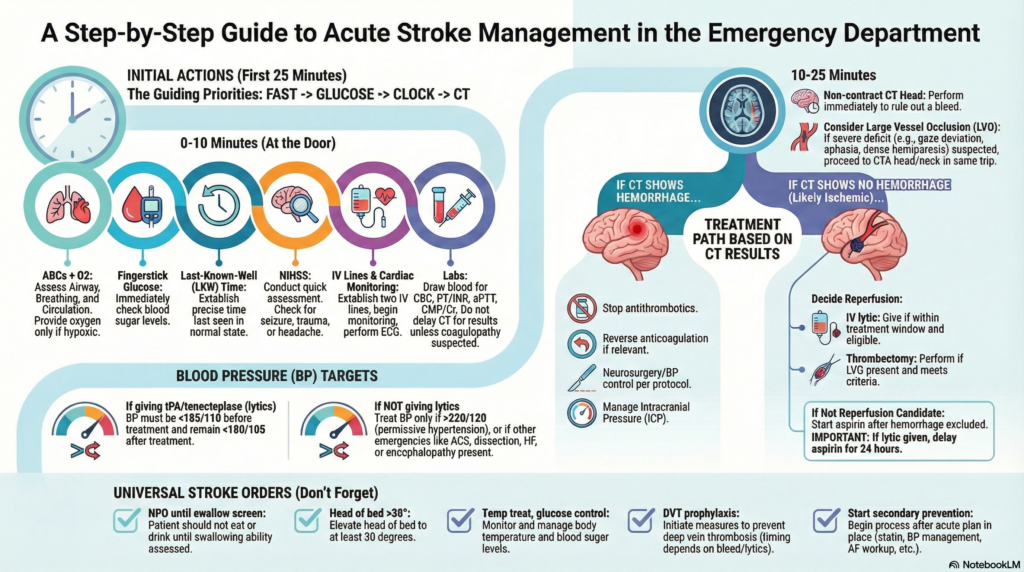
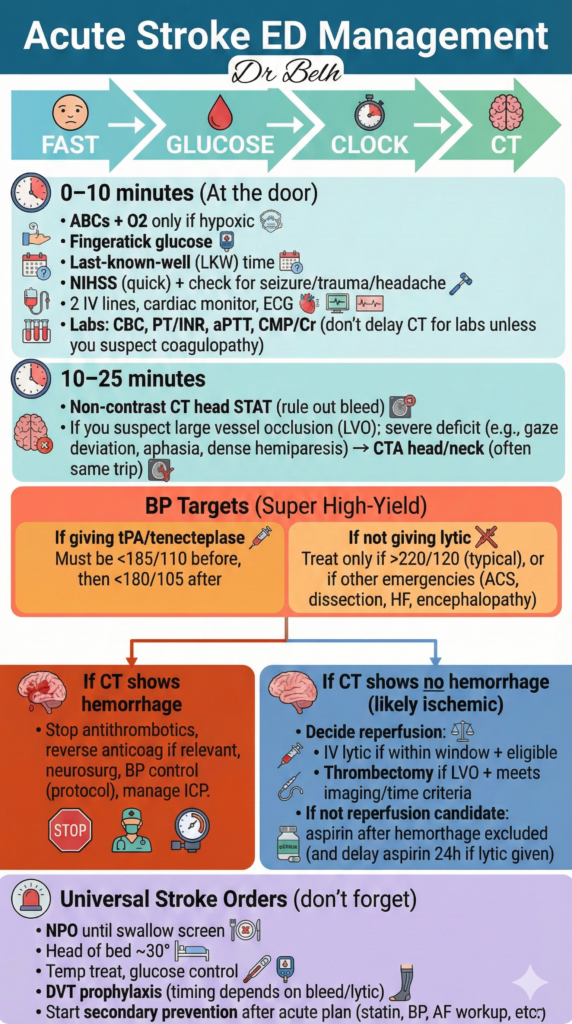
Quantify the deficit using the NIHSS and rule out mimics like hypoglycemia immediately.
Validate the ‘Last-Known-Well’ (LKW) time to define the eligibility window for tPA or TNK.
Execute the post-imaging pathway: Hemorrhage control vs. Reperfusion therapy.
Critical Timeline: Door-to-Needle Efficiency
Key Takeaways for Snippets
- LKW Time: The most critical factor for determining reperfusion eligibility.
- Blood Pressure Targets: <185/110 for lytics; <220/120 for non-lytic ischemic stroke.
- Glucose: Mandatory fingerstick to rule out metabolic mimics.
- Imaging: Non-contrast CT is the gold standard for ruling out hemorrhage.
Acute Stroke: The First Hour
| Category | Primary Intervention | BP Target |
|---|---|---|
| Ischemic (Lytic Candidate) | Reperfusion tPA/Tenecteplase | <185/110 mmHg |
| Ischemic (Non-Candidate) | Supportive Aspirin + Statins | <220/120 mmHg |
| Hemorrhagic | Control Reverse Anticoagulation | Aggressive (per neurosurgery) |
Clinical FAQ
1. Why check glucose first?
Hypoglycemia can induce focal neurological deficits that perfectly mimic a stroke.
2. Can we give aspirin before CT?
Never. Aspirin must be delayed until a CT has definitively ruled out hemorrhage.
3. What is the role of CTA?
CTA identifies Large Vessel Occlusions (LVOs) that may require mechanical thrombectomy.
4. Why wait 24h for aspirin post-lytics?
To minimize the risk of secondary intracranial hemorrhage during the high-risk window.
5. How do we manage ICP non-invasively?
Elevate the head of the bed to >30° to facilitate cerebral venous outflow.