Tinnitus is not an irreversible mechanical failure of the ear, but a categorization error of the Global Brain Network. The persistent sound originates from the auditory system but is sustained by the emotional centers of the brain. The clinical objective is not silence through suppression, but habituation through neuroplastic retraining.
Contents
Defining the Auditory Phantom
Clinically, tinnitus is the perception of sound in the absence of an external acoustic source. While often triggered by cochlear hair cell damage, the chronic condition is neurological. The brain compensates for lost input by increasing “gain” in the auditory cortex. This creates a feedback loop where the brain interprets internal neural noise as an external threat. Habituation is the biological process of reclassifying this signal from “threat” to “neutral background noise,” identical to how the brain filters out the sound of respiration or blood flow.
The Mechanistic Loop: Why It Persists
The persistence of tinnitus is governed by the interaction between the Auditory Cortex (processing) and the Amygdala (emotion/fear). When the Amygdala flags the sound as a threat, hyper-vigilance ensues.
The Distress Cycle
Autonomic Nervous Response
The Clinical Framework for Recovery
Effective treatment relies on breaking the connection between the auditory signal and the emotional reaction. We apply three core principles.
01. Observation
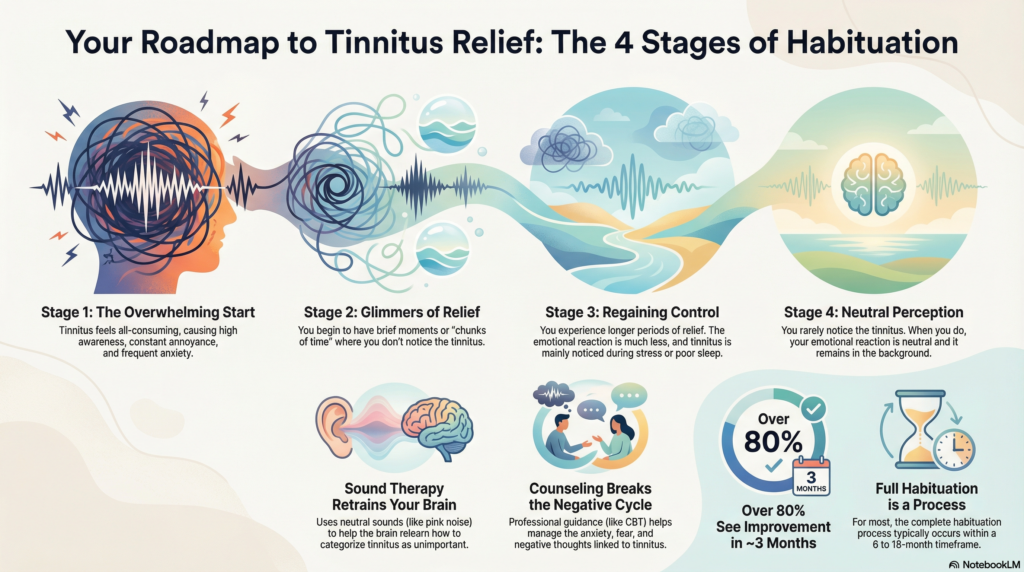
Identify the Stage. Recovery is non-linear. Patients move from “All-encompassing” (Stage 1) to “Intermittent” (Stage 2/3). Recognizing small breaks in perception is the first clinical sign of neuroplastic change.
02. Context
Sound Therapy “Mixing Point”. Use pink noise. Set volume to “mix” with the tinnitus, not mask it completely. This forces the brain to process both sounds simultaneously, reducing the signal-to-noise contrast.
03. Solution
Cognitive Reframing. Mechanical sound therapy must be paired with CBT. We must consciously relabel the sound from “Danger” to “Neutral Stimulus” to deactivate the Amygdala response.
The Neuroplastic Timeline
Month 0
High Distress
Month 3
Critical Shift (80% Relief)
Month 6-18
Full Habituation
Clinical Extraction Points
- The signal is real, the threat is not: Tinnitus is electrical activity misinterpreted by the emotional brain.
- Masking is counter-productive: Total silence prevents the brain from learning to filter the signal. Use the “Mixing Point.”
- Spikes are normal: Fluctuations in volume due to stress or sleep deprivation are expected and not a sign of regression.
- Consistency over intensity: Daily passive listening to sound therapy is more effective than sporadic effort.
Active vs. Habituated State
| Variable | Fight-or-Flight Mode | Habituated Mode |
|---|---|---|
| Amygdala Response | Active Threat | Neutral |
| Auditory Focus | Hyper-vigilant (Seeking sound) | Passive (Background filtering) |
| Emotional Impact | Anxiety, Panic, Despair | Indifference |
| Perception Example | “Snake Hissing” | “Refrigerator Humming” |
Visual Representation Prompt
Clinical FAQ
Does tinnitus ever go away completely?
For most, the electrical signal remains, but the perception vanishes. A habituated brain filters the sound out 99% of the time, functionally resulting in silence.
Why does my tinnitus spike in the morning?
Cortisol levels (stress hormone) are naturally highest upon waking. This heightens nervous system sensitivity, momentarily increasing the perceived volume of tinnitus.
Is silence dangerous for tinnitus?
Yes. Absolute silence increases the contrast between the environment and the internal sound, forcing the brain to focus on the tinnitus. Always maintain a low-level sound floor.
How long does habituation take?
Significant reduction in distress typically occurs within 3 months of proper protocol adherence. Complete habituation (Stage 4) typically requires 6 to 18 months.
Can hearing aids help if I don’t have severe hearing loss?
Yes. Hearing aids amplify external ambient frequencies, which naturally masks tinnitus and stimulates the auditory nerve, preventing the brain from compensating with phantom sounds.