Global Constat: Diabetes Mellitus represents a ubiquitous metabolic crisis unified by chronic hyperglycemia, yet driven by fundamentally divergent etiologies.
Problem: Clinical confusion between absolute insulin deficiency (Type 1) and relative deficiency combined with resistance (Type 2) leads to therapeutic mismanagement.
Resolution: This analysis delineates the distinct pathophysiological mechanisms, progression markers, and strategic management protocols for each phenotype.
Table of Contents
2.0 Etiological Definitions
Precise definitions are the bedrock of accurate diagnosis. We must distinguish between autoimmune destruction and metabolic dysfunction.
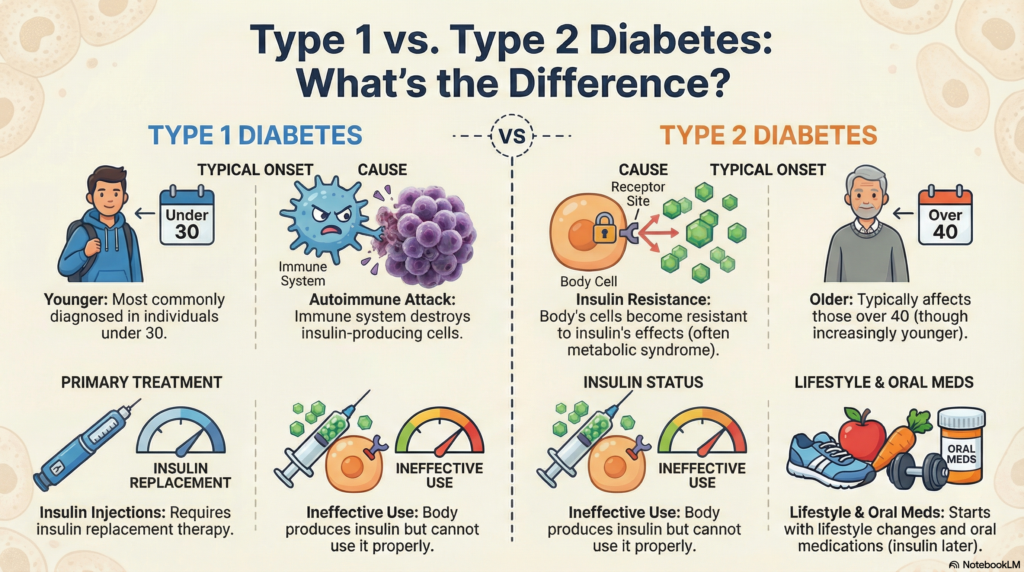
Type 1 Diabetes (T1DM)
An organ-specific autoimmune disorder characterized by the T-cell mediated destruction of pancreatic beta cells. This results in an absolute insulin deficiency, necessitating exogenous replacement for survival.
Type 2 Diabetes (T2DM)
A progressive metabolic condition initiated by peripheral insulin resistance. It evolves into relative insulin deficiency due to compensatory beta-cell exhaustion and amyloid deposition.
3.0 Mechanistic Analysis: The Pathophysiological Cascades
The progression from health to hyperglycemia follows two distinct linear pathways.
TYPE 1: The Autoimmune Cascade
TYPE 2: The Resistance Cascade
4.0 Dr. Belh Framework: The Clinical Triad
To navigate these pathologies effectively in a clinical setting, apply these three core principles.
1. Observation (The 3 Ps)
Regardless of etiology, hyperglycemia manifests universally. Look for Polyuria (osmotic diuresis), Polydipsia (hypothalamic thirst response), and Polyphagia (cellular starvation). In T1DM, add rapid weight loss.
2. Context (Biochemical Differentiation)
Do not guess; measure. C-Peptide is the arbiter. Low/Absent indicates T1DM (absolute failure). Elevated indicates early T2DM (hyperinsulinemic compensation). Confirm T1DM with Anti-GAD antibodies.
3. Solution (Targeted Therapy)
Match the therapy to the defect. T1DM requires basal-bolus insulin immediately. T2DM utilizes a step-wise approach: Lifestyle → Metformin → GLP1/SGLT2 → Insulin only upon exhaustion.
5.0 Key Points: Acute & Chronic Implications
- •
Acute Crisis Differentiation: T1DM predisposes to Diabetic Ketoacidosis (DKA) due to rapid ketogenesis. T2DM predisposes to Hyperosmolar Hyperglycemic Syndrome (HHS) as residual insulin suppresses massive ketone production. - •
Microvascular Damage: Both types lead to retinopathy, nephropathy, and neuropathy via non-enzymatic glycation of proteins in the basement membranes. - •
Macrovascular Risk: Accelerated atherosclerosis leads to CAD, Stroke, and PAD. This is often more advanced at diagnosis in T2DM due to the insidious onset.
6.0 Temporal Progression of Type 2 Diabetes
Unlike the rapid onset of T1DM, Type 2 follows a predictable chronological decay of beta-cell function.
Phase 1: Compensation
Insulin resistance begins. Normoglycemia is maintained by hyperinsulinemia (pancreatic overwork).
Phase 2: Pre-Diabetes
Beta cells fail to keep up. Postprandial spikes occur. Fasting glucose 100-125 mg/dL.
Phase 3: Overt Failure
Significant beta-cell mass loss (amyloidosis). Diagnosis confirmed (A1c > 6.5%). Microvascular damage begins.
7.0 Comparative Synthesis
| Feature | Type 1 Diabetes | Type 2 Diabetes |
|---|---|---|
| Primary Defect | Autoimmune Beta Cell Lysis | Insulin Resistance |
| Endogenous Insulin | Absent/Low | High then Low |
| Ketosis Prone | Yes (DKA) | Rare (Resistant) |
| Autoantibodies | Present (Anti-GAD, ICA) | Absent |
| Primary Treatment | Insulin Replacement | Diet, Metformin, Incretins |
Type 1 vs. Type 2 Differences.

8.0 Frequently Asked Questions
Can Type 2 Diabetes turn into Type 1?
No. They are distinct biological processes. However, a Type 2 patient can become “insulin dependent” if their beta cells burn out completely, mimicking the insulin requirement of Type 1, but the autoimmune etiology remains absent.
Why is weight loss a symptom of Type 1 but a cause of Type 2?
In Type 1, the lack of insulin causes the body to catabolize (break down) fat and muscle for energy, leading to rapid weight loss. In Type 2, excess adipose tissue releases pro-inflammatory cytokines that drive insulin resistance, making obesity a causal factor.
Is C-Peptide necessary for all diagnoses?
Not for classic presentations. However, it is essential in ambiguous cases, such as Latent Autoimmune Diabetes in Adults (LADA) or young patients with obesity, to distinguish between insulin deficiency (low C-peptide) and resistance (high C-peptide).
Why does DKA occur primarily in Type 1?
DKA requires a near-total absence of insulin to trigger unchecked ketogenesis. Type 2 patients usually retain enough endogenous insulin to suppress ketone production, preventing acidosis even if glucose levels are high.
What is the ‘Honeymoon Phase’ in Type 1 Diabetes?
This is a temporary period shortly after diagnosis where the remaining beta cells recover slightly, reducing insulin needs. It is transient, inevitably followed by total beta-cell loss.