Hyperglycemia in Type 2 diabetes is not a singular failure, but a complex breakdown of metabolic homeostasis. Effective management requires moving beyond “lowering sugar” to understanding the specific physiological levers we can pull. This analysis deconstructs the pharmacological playbook into five distinct, clinically validated strategies.
Table of Contents
Clinical Definition: Glucose Regulation
Hypoglycemic Pharmacotherapy refers to the strategic deployment of chemical agents designed to intervene in the body’s glucose modulation pathways. The objective is not merely to suppress blood glucose concentration, but to restore the equilibrium between hepatic production, peripheral uptake, and renal excretion. In a healthy state, this balance is maintained by the counter-regulatory hormones insulin (storage) and glucagon (release). Diabetes pathology represents the dissonance of this system.
Mechanistic Analysis: The Path of Dysfunction
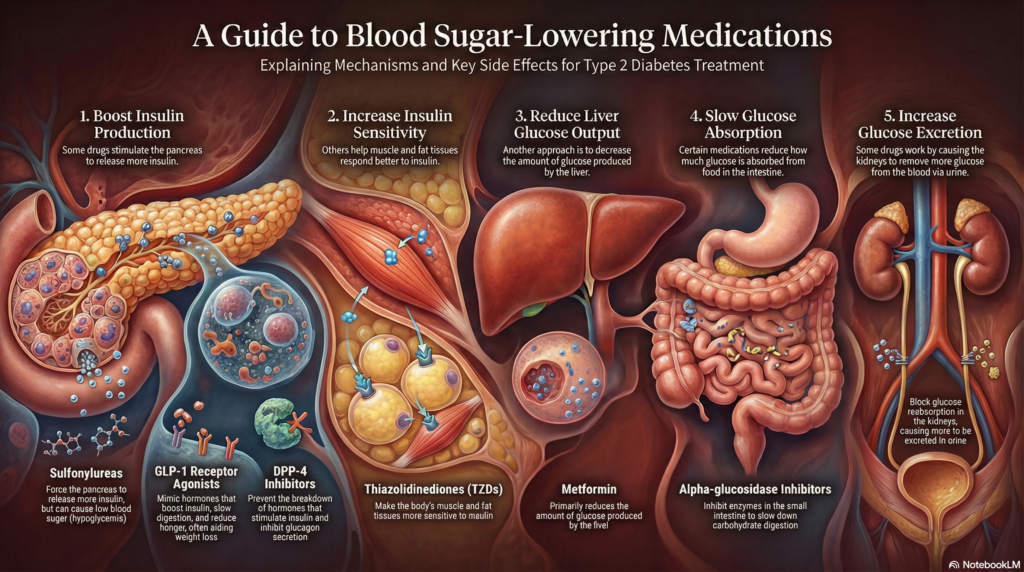
Understanding the target requires visualizing the physiological failure. The following flow illustrates where homeostasis breaks down and where intervention occurs.
Carbohydrates enter the gut.TARGET: Strategy 4 (Slow Absorption)
Glucose spikes. Pancreas signals Beta-cells.TARGET: Strategy 1 (Boost Insulin)
Liver overproduces glucose. Muscles refuse it.TARGET: Strategy 2 & 3 (Sensitivity & Output)
Kidneys reabsorb excess glucose.TARGET: Strategy 5 (Force Excretion)
Applied Clinical Approach: The Dr. Belh Framework
To navigate these strategies effectively, we apply a tripartite framework: Observation, Contextualization, and Targeted Solution.
1. Observation
Hyperglycemia is the symptom, not the root cause. We must observe the patient’s specific metabolic profile (e.g., obese vs. lean, post-prandial spikes vs. fasting highs).
2. Context
Identify the organ system failure. Is the pancreas exhausted? Is the liver deregulated? Is the gut absorbing too rapidly? Context drives drug selection.
3. Solution
Select the pharmacological agent that maps directly to the context. Avoid redundancy; aim for complementary mechanisms of action.
Deep Dive: The 5 Strategic Pillars
Strategy 1: Augmenting Insulin Supply (Pancreatic Stimulation)
This approach addresses insulin deficiency by compelling pancreatic beta-cells to increase output.
- Sulfonylureas & Meglitinides: Direct stimulation of insulin release. Warning: High risk of hypoglycemia as release occurs regardless of glucose level.
- GLP-1 Agonists & DPP-4 Inhibitors: The “Smart” stimulators. They utilize the incretin pathway to boost insulin only when food is present, reducing hypoglycemia risk while suppressing glucagon.
Strategy 2: Enhancing Peripheral Sensitivity (The Reception)
If the key (insulin) exists but the lock (receptor) is jammed, more insulin isn’t the only answer. Thiazolidinediones activate PPAR-gamma receptors, fundamentally altering gene expression to make muscle and adipose tissue receptive to glucose uptake.
Strategy 3: Suppressing Hepatic Output (The Factory)
In Type 2 diabetes, the liver acts as if the body is starving, pumping out glucose continuously. Metformin, the gold standard, acts here. It signals the liver to cease gluconeogenesis (new sugar creation), effectively turning off the tap.
Strategy 4: Retarding Intestinal Absorption (The Intake)
By inhibiting alpha-glucosidase enzymes, drugs in this class act as a traffic warden in the gut. They delay carbohydrate breakdown, flattening the post-prandial glucose spike. It creates a “trickle” effect rather than a flood.
Strategy 5: Inducing Renal Excretion (The Release Valve)
The newest strategy involves SGLT2 Inhibitors. Normally, kidneys aggressively reabsorb glucose. These drugs block that reabsorption, allowing the body to flush excess glucose out via urine. It is a hemodynamic and caloric offloading mechanism.
Therapeutic Efficacy Timeline
Immediate
Insulin Secretion
(Sulfonylureas)
Days to Weeks
Hepatic Control
(Metformin)
Weeks to Months
Sensitivity Shift
(TZDs / GLP-1 Weight Loss)
Clinical Extraction Zone (Key Points)
- Redundancy is futile: Combining two drugs that both stimulate insulin secretion (e.g., Sulfonylurea + Meglitinide) increases risk without benefit.
- Organ Protection: SGLT2 inhibitors and GLP-1 agonists are now preferred for their cardioprotective and renal-protective properties, beyond glucose control.
- The Metformin Base: Unless contraindicated, suppressing hepatic output remains the foundational first step.
- Hypoglycemia Awareness: Only strategies that force insulin independent of glucose (Strategy 1A) carry significant hypo risks.
Synthesis: Mechanism Matrix
| Strategy | Primary Drug Class | Primary Organ | Weight Impact |
|---|---|---|---|
| Boost Insulin | Sulfonylureas / GLP-1 | Pancreas | Loss (GLP-1) / Gain (Sulfon) |
| Sensitivity | Thiazolidinediones | Muscle / Fat | Gain |
| Reduce Output | Metformin | Liver | Neutral/Loss |
| Slow Absorption | Alpha-glucosidase Inh. | Intestine | Neutral |
| Increase Excretion | SGLT2 Inhibitors | Kidney | Loss |
Visual Reference (Image Prompt)
Clinical FAQ
Why is Metformin usually the first choice?
It targets the root cause (excess liver production), has a high safety profile, does not cause hypoglycemia, and is weight-neutral.
Can SGLT2 inhibitors damage the kidneys?
Paradoxically, while they act on the kidneys, they are proven to slow the progression of chronic kidney disease in the long term, though acute checks are required.
Why do GLP-1 agonists cause weight loss?
They slow gastric emptying (making you feel full physically) and act on the brain’s satiety centers (making you feel full mentally).
Are Sulfonylureas outdated?
They are older and carry higher risks, but remain effective and cost-efficient. They are often used when newer agents are inaccessible.
What happens if oral medications fail?
If the 5 strategies cannot overcome insulin resistance or beta-cell burnout, exogenous insulin therapy (replacement) becomes the necessary 6th strategy.