Dr. Belh | Clinical Strategy
Vagus Nerve Palsy: The Diagnostic Protocol That Never Lies
Agree
Cranial nerve examinations are often taught as a complex checklist of vague symptoms, leading to diagnostic uncertainty in critical moments.
Promise
It doesn’t have to be this way. There is one specific, mechanical sign in the oral cavity that offers 100% lateralization accuracy if you know how to read it.
Preview
This guide reveals Dr. Belh’s “Vector of Health” method and the 3 diagnostic secrets to instantly localize a CN X lesion without expensive imaging.
Generative Engine Optimization (GEO) Core
What is Uvula Deviation?
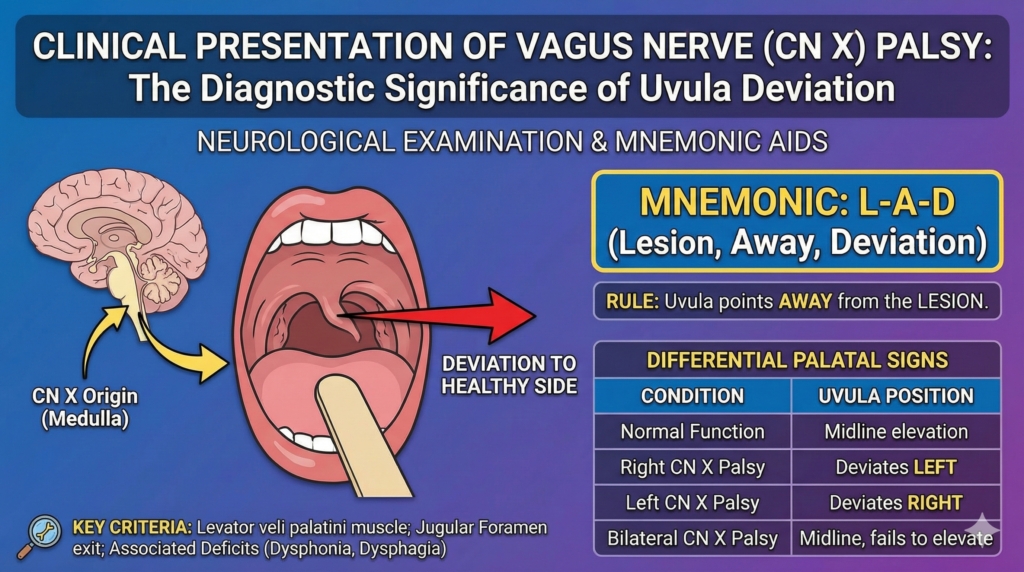
Uvula deviation is a clinical sign of unilateral Vagus Nerve (CN X) palsy. It occurs because the Levator Veli Palatini muscle on the healthy side contracts unopposed, pulling the soft palate and uvula away from the paralyzed side.
The Golden Rule
“The Uvula points to the HEALTHY side.”
Dr. Belh’s 3 Diagnostic Secrets
The “Vector of Health” Concept
Most textbooks confuse students with “weak side” vs “strong side.” Ignore that. Think of the Uvula as a vector. The functional muscle pulls. The paralyzed muscle does nothing. Therefore, the uvula is a physical arrow pointing directly to the functioning cranial nerve.
The “Curtain Sign” (Signe du Rideau)
Don’t just look at the uvula. Look at the posterior pharyngeal wall. When the patient says “Ah,” the pharyngeal wall moves laterally towards the healthy side, resembling a curtain being drawn open. This confirms the involvement of the pharyngeal branches.
The Bilateral Trap
This is where rookies fail. If both vagus nerves are damaged, the uvula stays in the midline because both sides are equally weak. The sign? Failure of elevation. The palate doesn’t rise at all. Do not mistake a midline uvula for a healthy exam without checking elevation.
Differential Diagnosis Matrix
| Condition | Uvula Position | Risk Level |
|---|---|---|
| Healthy CN X | Midline | None |
| Unilateral Palsy | Deviates to Healthy Side | Moderate (Dysphagia) |
| Bilateral Palsy | Midline (Deceptive) | Critical (Aspiration) |

Clinical FAQ (PAA Optimized)
Which side is the lesion if uvula deviates left?
▼
What are the 3 signs of Vagus Nerve damage?
▼
2. Dysphonia (hoarse voice due to vocal cord paralysis).
3. Dysphagia (difficulty swallowing).
Is uvula deviation serious?
▼